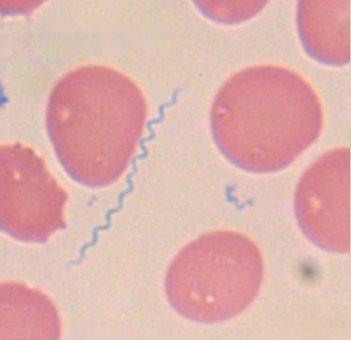
Borrelia burgdorferi (Bb) is the main cause of Lyme disease (LD) in the U.S. (Borrelia afzelii and Borrelia garinii cause most European cases.) It is a spirochete. Spirochetes belong to a phylum of distinctive Gram-negative bacteria that have long, helically coiled cells. Spirochetes are distinguished from other bacterial phyla by the location of their flagella (sometimes called axial filaments), which run lengthwise between the cell wall and outer membrane. Other diseases are caused by spirochetes, for example, syphilis is caused by the spirochete Treponema pallidum.
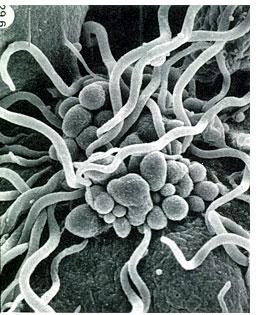
Bb is the most genetically complex bacterium identified to date. It contains 132 functional genes, compared to the syphilis spirochete's 22. Ninety percent of these genes are novel to all bacteria. Bb contains 21 plasmids, more than any other bacteria. This characteristic allows the organism to be highly adaptive to its environment, with the ability to survive in a number of different hosts. Under stress, in the presence of antibiotics or cerebrospinal fluid (CSF), the organism changes morphology. Currently identified morphological variations include spirochetal form (coiled and uncoiled), cystic form, blebs and granules, and cell wall-deficient (L-form). They enable the organism to become latent for long periods of time, resist treatment, and evade immune recognition. (source)
 |
 |
 |
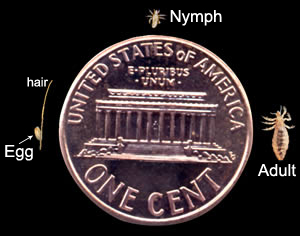
| While only 0.2-0.3 microns wide, Bb's cell length may exceed 15 microns. (Source) |
Bartonellosis is caused by a genus of Gram-negative bacteria called Bartonella. At least eight species are
known to infect humans. Different species cause different diseases. For example, Bartonella henselae causes
cat scratch disease, Bartonella bacilliformis causes Carrion's disease, and Bartonella quintana causes
trench fever. Other species such as Bartonella vinsonii subspecies berkhoffii have an affinity for
red blood cells (RBCs) and endothelial cells (cells that line the insides of our blood vessels)
(source). This causes intravascular disease,
which hinders nutrient and oxygen delivery to tissues, resulting in fatigue and pain, as well as cognitive and
emotional problems. Bartonella actually enters RBCs (source1
source2). Bartonella's affinity for RBCs can be at least partly explained by
its need for a substance called hemin, which is plentiful in RBCs.
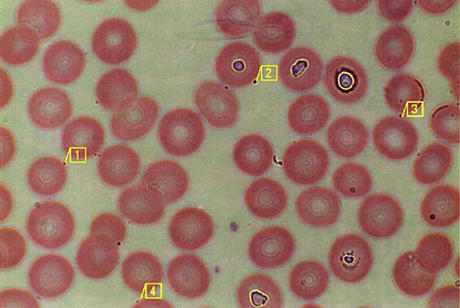
Inside RBCs the bacteria multiply, and when a biting insect takes blood from
the host, it picks up infected RBCs, thereby becoming a carrier that can infect other animals or
humans. At least one Bartonella species secretes a substance called deformin that causes RBCs
to become misshapen
(source).
Intracellular Bartonella infection starts with the secretion of adhesins that allow the bacteria to adhere to target cells (normally RBCs and endothelial cells, but possibly macrophages as well). Then the bacteria secrete effector proteins and/or DNA into those cells via the type IV secretion system. The effector proteins subvert multiple cellular functions to the benefit of the infecting pathogen. Eventually bacteria enter the target cells, where they replicate until there are an average of eight bacteria per target cell, and they remain there for the life of the cell (the exception is Bartonella bacilliformis, which typically kills RBCs). (source1 source2 source3)
While a significant portion of Bartonella cells in an infected organism are found inside RBCs, it appears that every 3-6 days there is a new RBC infection wave. This could indicate that the primary niche is another type of cell (perhaps endothelial cells, or certain bone marrow cells such as angioblasts and erythroblasts) from which new bacteria emerge every few days. (source1 source2)
Bartonellosis is possibly the most common tick-borne disease (source). How can this be, when most people have heard of Lyme disease and so few have heard of bartonellosis? Remember that "Lyme disease" is a lay term while bartonellosis is technical. Lyme disease is sometimes referred to in the medical community as borreliosis (because it is caused by a Borrelia bacterium). How many people have heard of borreliosis? Lyme disease is much easier to remember. Similarly, people are familiar with lay terms for Bartonella-caused illnesses such as cat scratch disease and trench fever. However, since many new Bartonella species have been discovered in recent years, no lay terms have been invented to refer to their diseases, so they are referred to simply as bartonellosis. Furthermore, the bacterium that causes Lyme disease was identified in 1982, and tests to detect it have been around for a long time. Most Bartonella species, on the other hand, were not discovered until many years later, so they have gone largely undetected and news of their existence has not spread nearly as much. As for how bartonellosis can be more prevalent than Lyme disease, it is thought that Bartonella, as opposed to Borrelia burgdorferi, is virtually everywhere except countries near the cold northern and southern poles (source).
 |
Biting arthropods
can transmit several parasites and thus infect us with several diseases.
The most well-known vectors are ticks,
which are arachnids, not insects.
(Insects compose a
class within the
phylum
arthropoda.)
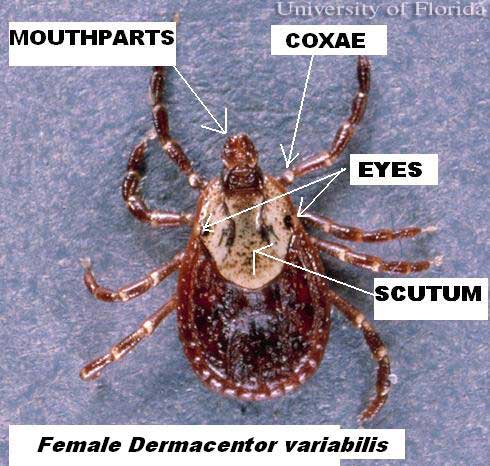
North American ticks include the black-legged tick or deer tick (Ixodes scapularis, formerly Ixodes dammini),
the western black-legged tick (Ixodes pacificus), the brown dog tick (Rhipicephalus sanguineus) and the
American dog tick (Dermacentor variabilis). There is some debate about some tick species. For example,
one source
says that the Lone Star tick (Amblyomma americanum) causes
LD while others such as this one
say that it
doesn't. The bottom line is that all ticks should be avoided because nobody except experienced
entomologists can tell the species apart, and even if a tick doesn't contain Bb or Bartonella, it could
very well carry any of the other vector-related pathogens.
LD is the fastest growing vector-borne disease, due to suburban sprawl (which brings people close
to forests), increasing deer populations, ticks being carried by migratory birds, and other factors
(source). Additionally, since LD is carried by rodents, a decrease in numbers
of foxes (which prey on rodents) might be contributing to the spread of LD
(source).
Alarmingly, Bb and Bartonella can be passed from mothers to their unborn children, and also to blood transfusion recipients. (source)
Bb and Bartonella are two extremely difficult organisms to detect. Identification is not a simple matter of
having blood drawn and seeing the organism or specific antibodies in the sample. If it were that easy,
everyone could be easily diagnosed. The bacteria have an affinity for bodily tissues rather than fluids.
They can be difficult to culture from tissue samples. Sometimes, but not always, antibodies are found.
Enzyme-linked immunosorbent assay (ELISA) is used to detect
antibodies, but it is not always accurate. Another test,
Western blot, is used to detect specific proteins,
but this test is also not always accurate. Even when these two tests are run, a full one-third of cases go
undetected. There are also occasional false positives. Why are these tests so inaccurate?
For a number of reasons:
A CD-57 test might be helpful.
Chronic Bb infections are known to decrease the quantity of the CD-57 subset of the natural killer cells.
While other infections can depress the immune system, it is believed that only Bb will depress the CD-57.
(source)
If an infected person is lucky, he/she will develop a skin rash called
erythema migrans. This will alert
the victim that he/she has been infected so that prompt antibiotic treatment can kill the bacteria before
it spreads throughout the body. Unfortunately this only happens about half the time,
and victims are not aware that anything is wrong until the illness is systemic.
Bb can inhibit the immune system, activate inflammatory processes, and trigger autoimmunity by mimicking
bodily cells. The result is pains, aches and weakness. Bb can adhere to a number of cell types,
including glia (cells that support, feed and insulate neurons) and the interior surface of blood vessels.
In advanced LD, the spirochete crosses the blood-brain barrier (BBB). This is termed
neuroborreliosis. The antibiotic minocycline
is indicated because it, too, crosses the BBB. Minocycline can be neuroprotective, possibly by inhibiting
inflammatory substances that damage or kill brain cells (source1
source2 source3).
Because Bartonella bacteria can burrow into our cells, they avoid our immune defenses, and the only
antibiotics that have any chance of killing them are ones that also penetrate our cell walls.
Azithromycin and
rifampin are often preferred. Rifampin is very good at
infiltrating almost all of our bodily cells, as well as the CSF because it crosses
the BBB. Rifampin can cause liver damage
(source).
It increases the liver's production of CYP3A4,
which increases the rate at which the liver metabolizes some other drugs and thereby necessitates
higher doses of them. (example)
Bartonella might or might not cross the BBB, but even if it doesn't, damage to brain tissue could occur
via imbalances induced by the organism. For example, induction of high systemic levels of cytokines
such as tumor necrosis factor alpha, produced in response to infection, could lead to temporary or permanent
damage to brain tissue.
Bartonella can mess with the immune system by secreting chemicals that turn off immunity and immune defense inflammation.
For example, a lipopolysaccharide produced by Bartonella is a potent antagonist of Toll-like receptor 4 (TLR4), as it inhibits both RNA transcription and the release of tumor necrosis factor alpha, interleukin IL-1 beta, and IL-6 by E. coli
lipopolysaccharide in human monocytes. This Bartonella lipopolysaccharide is so powerful that it is being looked at as a treatment for autoimmune diseases. (source).
The specific areas of the body affected by Bb and Bartonella very widely. Just about any joint or muscle can
become achy, painful, tender, weak, and/or easily fatigued. Other symptoms are possible, including but not
limited to fever, loss of appetite, dizziness, and loss of libido.
Both Bb and Bartonella, when they affect the brain, cause irritability, depression, cognitive impairment,
short-term memory loss, and other mental problems. The psychological effects can be dramatic, causing
victims to become easily upset and angry (source).
One culprit is cerebral hypoperfusion (lack of oxygen
and nutrient delivery) to the white matter of the brain. This is usually detected by single photon emission
computed tomography (SPECT)
or magnetic resonance imaging (MRI).
The white matter lesions and the associated symptoms are common in demyelinating or inflammatory disorders such
as multiple sclerosis and lupus, hence Lyme or bartonellosis symptoms can cause erroneous diagnoses.
Furthermore, it is possible to have Bartonella-induced multiple sclerosis,
so while a diagnosis of multiple sclerosis might be correct, medical personnel making the diagnosis might not
know what is causing it and therefore will not know that it is curable.
Bb and Bartonella can cause RBCs to stick together (any inflammation can cause this via the body's increased
production of fibrinogen).
This makes it difficult for RBCs to pass through
capillaries, which are only as wide as a single RBC. This contributes to hypoperfusion and the associated
fatigue and psychological problems.
People who don't know they have one of these infections, but experience symptoms, are often diagnosed with
"fibromyalgia" or
"chronic fatigue syndrome",
both of which have "unknown" causes and are "incurable".
Treatment is focused merely on easing the symptoms via pain killers, steroids, behavioral therapy, exercise,
antidepressants, and even antifungals. This misdiagnosis not only causes the infection to go intreated,
but can also exacerbate it if steroids are given because steroids weaken immune defenses and the administration
of steroids during an active infection can cause permanent damage (source).
The effects of both LD and bartonellosis in the body are profound and widespread because vascular
damage and inflammation can affect every bodily system. For example, organs such as the adrenals, brain and
thyroid, which produce hormones, can be disrupted, causing hormone imbalances that result in many physical
and psychological symptoms such as weight gain or loss, anxiety, weakness, loss of libido,
short temper, and hair loss. Additionally, the inflammatory cascade can
block cellular hormone receptors, resulting in
insulin resistance
and hypothyroidism despite normal
T3 and
T4 levels.
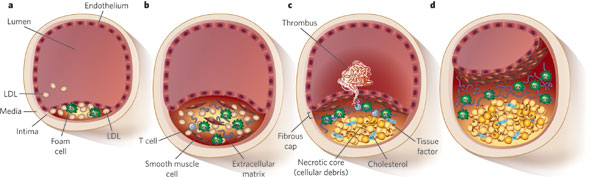
Inflammation of the inner surface of blood vessels (the endothelium) is the first step in
atherosclerosis, so Bb, Bartonella, or any other pathogen can cause heart disease and stroke.
Once arterial endothelium is damaged, monocytes (a type of white blood cell) adhere to the endothelium
and become macrophages (cells that rid the body of foreign cells by engulfing them). The endothelium
and macrophages release free radicals, which oxidize the polyunsaturated fat portion of low density
lipoproteins (LDLs), creating oxidized LDL (OxLDL). The macrophages engorge themselves with OxLDL and
take on a foamy appearance, at which point they are referred to as foam cells. They form yellow
fatty streaks. Platelets adhere and aggregate at the site. This causes the artery to secrete collagen,
elastin and proteoglycans, leading to the formation of fibrous tissue, called a plaque,
lesion or atheroma.
(Note: Atherosclerosis happens only in arteries, not in veins, because arterial smooth muscle cells have
binding sites for a component of LDL called apoB-100.)
Since many of the symptoms of LD and bartonellosis are similar, it is very common to assume that a victim has LD,
since LD is the most commonly known tick-borne disease. Many sufferers actually have bartonellosis, but since
most people have never heard of it, LD is used as a general term. It is important for people to be made aware
that LD is but one of several vector-borne diseases.
How can one differentiate between LD and bartonellosis? Aside from a conclusive blood test, symptomatology can
help. Although many symptoms of these two diseases are similar, a few differ. For example, bartonellosis
sufferers sometimes get erythematous papules, which are red splotches or slightly raised red spots
that may appear on the limbs, head or neck. Painful soles are also specific to bartonellosis. LD often causes
joint aches, while bartonellosis is more likely to cause muscle weakness and bone pain. LD often causes sleepiness,
while bartonellosis is more likely to cause insomnia.
The psychological effects can be devastating to relationships. Friends, family members and significant others
have abandoned loved ones when their hypersensitivity has caused them to become critical and aggressive toward
others. Bartonella in particular can cause victims to become unjustly angry at others, and this has brought
about the term "Bartonella rage".
Additionally, the inability to engage in social situations has left victims alone and frustrated. Victims
can become so worn down and hopeless after several months without relief that they may become depressed and suicidal.
It is important for loved ones to understand that it is the illness, not the person, that is being difficult to
deal with. It is ironic that people can be very understanding when loved ones are afflicted with other brain
disorders such as mental retardation, clinical depression and Alzheimer's disease, but when it comes to
psychiatric LD/bartonellosis,
they lose sight of the disease and ascribe difficult behavior to the individual rather than the disease. This
might cause them to lash back verbally at, or walk out on, their afflicted loved one, which makes the victim
feel even worse.
The knowledge that
a loved one's behavior is caused by a physical disorder often takes a back seat when one has to deal with
undeserved criticism and lack of affection every day for months on end. One's ability to be patient and
understanding during this difficult time depends on a number of factors. Some people are naturally patient and/or
able to let verbal abuse bounce off them; others are short-tempered and/or easily hurt by words. Most of us fall
somewhere in the middle.
Perhaps an account of my personal experience will help victims' loved ones understand and cope better. In June 2007
I met a woman with whom I fell madly in love. We had an absolutely heavenly relationship. Around that time she
was diagnosed with LD. An MRI of her brain showed that she had been infected for some time, but for how long
we did not know. She underwent months of antibiotic treatment. The psychological effects weren't bad
enough to affect our relationship, but she did often overreact when her daughter misbehaved. By the summer of 2008
antibiotics had rid her of Bb, but
her behavior toward me took a turn for the worse: she became critical of many little things that had never bothered
her before, and she became less affectionate. In December that year she was tested for Bartonella, since it is not
uncommon for LD patients to have coinfections that remain dormant until the Bb is eradicated. The following month
her doctor received a positive test result from a lab in North Carolina, so it was bartonellosis rather than
LD that was affecting her behavior. For some reason he did not notify her of the positive test.
In the ensuing months her condition did not improve. In fact, at times she got
downright belligerent. It was very sad, frustrating and angering to watch my significant other turn into a
monster. Even though I knew that it was probably some disease causing her behavior (I didn't know that it was
bartonellosis but suspected that it was either that or perhaps her LD had relapsed), it still hurt to have her criticize and yell
at me. I walked out on her several times (I used to sleep at her house most of the time, but we maintained
separate houses), and each time I came back we would make up and
she would be very sorry for her behavior, but within a few days she would give me the same harsh treatment.
After an emotional meltdown in October 2009 she finally rescheduled another appointment, where she learned of her
Bartonella infection. She started antibiotic
treatment (azithromycin and rifampin). Since it takes a long time to eradicate the bacteria (this will be
explained in the Treatment section), her
mood remained unpleasant. Both her brain and her hormones were adversely affected, and this wreaked havoc on her
psyche. Rarely a day went by when she didn't criticize me about something, and not just normal relationship criticism
either. Everything about me bothered her: my eating habits, my favorite TV shows, the way I cut my hair. When
I'd wash dishes she'd get upset because I used "too much soap" on the sponge. Her hormonal imbalance exacerbated her
PMS, causing her mood and behavior to become almost unbearable for two weeks per month. Her once strong libido all
but vanished. Even though I knew on an intellectual level
that this wasn't the real her, on an emotional level I started to wonder whether it was the disease causing her behavior after
all. A lot of relationships start out great but eventually turn sour, so maybe this was happening to us.
Was our first year together merely the
"honeymoon phase"? Had the novelty worn off? Was she now taking me for granted? Were her infections merely coincidental
to her behavioral change?
I developed a lot of resentment and walked out on her a few more times in the following months. Shortly before Memorial
Day Weekend 2010 I had reached my breaking point. One night she was particularly nasty toward me,
and the next day I told her that I needed a mental health break. After nearly two years of being her whipping boy I had
had enough. I knew that she needed my support, but I would be of no use to anyone if I ended up in an asylum. During the next
three weeks we remained friends and saw each other at social events. She
started to improve emotionally, and as her head cleared she was very remorseful about the way she had treated me.
Her mood and her libido
were greatly improved. In fact, she seemed for the first time in two years to be her old self: she was very pleasant, little
things didn't bother her, and we made love more times in the following month than we had
all year. Even when her PMS eventually kicked in, she was able to handle it and did
not become overly sensitive or critical.
One very important lesson that I learned from all this is not to lose hope.
If your significant other is ill, don't lose sight of the person that
he/she used to be. This doesn't mean that you must stand there and take whatever abuse your loved one dishes out, but it does
mean that the relationship/marriage does not have to end.
Another lesson that I learned is that the one with the infection is not the only victim; the
people close to the victim become victims as well. Although the one with the bacteria has needs, this person's loved
ones have needs too. If you have an infected loved one, take care of your emotional needs. Even though your basic
personality type and tolerance for harsh treatment cannot be changed, there are several other factors that you can control:
Much controversy surrounds the idea of chronic Lyme disease. There are certainly people who have had Lyme and/or other
vector-borne diseases for a long time and have suffered many symptoms. However, a significant number of people in
the medical community believe that some chronic illnesses that are not Bb-related are misdiagnosed as "chronic
Lyme disease". They contend that some sufferers were never infected with Bb, and that others were infected with
Bb at one time but the spirochete has been eliminated and they are now suffering from "post-Lyme disease syndrome"
(source1
source2). Studies such as
this one cast doubt on the prevalence of chronic LD, but it could be that
either the detection methods failed for any of the reasons described
above; or the "chronic Lyme" was really
chronic bartonellosis, or chronic ehrlichiosis, or chronic babesiosis. All of these pathogens should
be tested for before the possibility of infection is dismissed, and also to make sure that the right pathogen
is identified so that the right antibiotic treatment is administered.
Lyme disease is one of the most controversial illnesses in the history of medicine
(source).
The controversy over chronic LD has become fierce and political. On one side are the believers, such as
the International Lyme and Associated Diseases Society (ILADS). On the other side
are the non-believers, who say that long regimens of antibiotics are unnecessary and even dangerous
(source).
This group includes the Infectious Diseases Society of America (IDSA).
Many insurance companies are in the latter camp
(source), perhaps in order to reduce costs rather
than to provide needed treatment. Some doctors have even been prosecuted and had their licenses
suspended for treating Lyme patients in a manner that departs from what medical boards define as
"acceptable and prevailing standards" (example).
There is only one way to cure LD and bartonellosis: antibiotics. But not just any antibiotics.
The key to eradicating any pathogen is the right medication(s) for the right amount of time.
Often times even when
Bb and/or Bartonella are detected, the wrong type of antibiotic is prescribed, and/or the antibiotic is not given
for a long enough duration. Leaving even a few live bacterial cells can allow later repopulation and
relapse, possibly with antibiotic-resistant bacteria.
Treatment must be obtained from a doctor who is properly educated
about vector-borne illnesses. Often the acronym LLMD (Lyme-literate MD) is used to describe such
a person, but since several coinfections can occur with Lyme disease, LLMD is a misnomer. A better acronym
might be VBILMD (vector-borne illness-literate MD).
Which antibiotics are appropriate, dosage, and how long to administer them for, depend on many
factors such as which bacteria are present, whether they have gone systemic, and whether they have reached
the brain/CSF, as well as the patient's age and weight. Only a medical professional who is educated
specifically about
LD and bartonellosis can deliver proper treatment. General practitioners often go with a
"standard" antibiotic regimen, which might be ineffective.
Ironically, I was bitten by a tick in May 2011. My primary care physician would not give me
prophylactic antibiotic therapy due to the IDSA's guidelines, which state:
Since it had been more than 72 hours since the bite, I did not qualify for prophylactic treatment. If I had presented with symptoms, such as joint pain or
erythema migrans, I would have been put on a more aggressive antibiotic regimen, but since I did not have symptoms,
I received no treatment at all. So, for peace of mind I went to a VBILMD, who, like many VBILMDs, does
not take insurance, and I ended up paying several hundred dollars out of pocket.
Coinfections can greatly complicate treatment. For example, let's say a patient has both Bb and Bartonella.
If the doctor is only aware of the Bb and successfully treats it, then the Bartonella might cause symptoms
that are erroneously attributed to the Bb. The doctor might continue to treat the (nonexistent) Bb with an
antibiotic that is effective against Bb but ineffective against Bartonella, or he/she might claim that the
patient merely has "post-Lyme
disease syndrome" and discontinue antibiotics altogether, so that the patient will continue to live with
an undiagnosed infection. This is why it is so crucial to get treatment from a VBILMD.
Often more than one antibiotic is required even if a patient is infected with only one bacterium. For example,
since Bb can take so many forms, a particular antibiotic might be effective against one form but not another, so
a single antibiotic might kill only a portion of the bacterial population. One such case involved my former
girlfriend, who in 2007
was given a 30-day course of intravenous ceftriaxone
via a
peripherally inserted central catheter in her arm.
Her symptoms eased for a while, but she later relapsed. It turns out that
cephalosporins such as ceftriaxone do not
kill the cystic form of Bb (source).
Bb has the ability to make cystic forms when exposed to
antibiotics commonly used for treating Lyme disease.
The effectiveness of most antibiotics requires active metabolism by the bacteria, so while active spirochetes might be killed, the cysts remain unaffected. Once antibiotic treatment is over, the cysts can reconvert to normal mobile spirochetes, causing a reactivation of the disease after an illusory cure. (Author of source requested that her material be withheld from this site.)
One antibiotic that can be effective against the cyst form is metronidazole (source1 source2). Anyway, my former girlfriend started minocycline after her relapse, and within eight months she was Bb-free.
It has been suggested that Bb can produce beta-lactamase, which degrades
beta-lactam antibiotics such as
cephalosporins and penicillins (source). Perhaps this is why ceftriaxone is not
completely effective against Bb. The addition of a beta-lactamase inhibitor such as
sulbactam or
clavulanate
can greatly increase the efficacy of beta-lactam antibiotics (for example,
Augmentin is a mixture of
amoxicillin and clavulanate).
Another mechanism by which Bb might resist penicillin is the production of penicillin-binding proteins
(source). Clavulanate might be able to bind to them, thus reducung Bb's resistance
to penicillin whether or not the cells produce beta-lactamase (source).
Antibiotic treatment can take many months if LD and bartonellosis are not caught early. Why should this be,
when other infections such as strep throat can be cleared up within a week or two? One reason is the
longer life cycle. Bartonella takes 24 hours to divide, and Bb takes anywhere from 12 hours to 7 days --
much longer than that of Streptococcus pyogenes (the bacterium that causes strep throat), which takes
anywhere from 20 minutes to 8 hours to divide. Since most antibiotics work
best while bacteria are replicating, a longer replication cycle necessitates a longer treatment course.
(source1
source2)
Even so, why should treatment take so much longer than the replication time? Aren't all bacteria
killed once they try to replicate? Unfortunately, no. Experts do not yet know why. Perhaps lethal antibiotic
concentrations are not reached in all infected cells.
Other medications might be needed during antibiotic treatment. For example, since there can be temporary
hypothyroidism from thyroid disruption, T3 and/or T4 supplements might be needed. These may relieve some
of the aches, weakness and/or depression that hypothyroidism can cause. Mental problems such as depression,
ADD/ADHD and irritability can be treated by a psychiatrist with
SSRIs,
SNRIs,
NDRIs and/or
sedatives.
Note that problems such as ADD/ADHD can be caused by things other than infections. For information about
symptoms of and treatment for ADD/ADHD, click
here.
Once antibiotic treatment begins, patients often experience the
Herxheimer reaction, which occurs when
large quantities of toxins are released into the body as bacteria die from antibiotic treatment.
Typically this occurs faster than the body can remove the toxins. "Herxing" is manifested by fever,
chills, headache, myalgia (muscle pain), etc. It can last for as little as a few hours or, in the case of
LD and bartonellosis, months.
One might ask, "What specific toxins do bacteria release when they die?" Little data is available on
this matter, because there is currently no reliable test for identifying these toxins. The existence
of toxins is usually inferred from symptoms and the presence of
cytokines, hormone resistance, etc.
One possible toxin produced by Bb is ammonia. Ammonia can cause "leaky brain syndrome" by
damaging the BBB, thus enabling larger molecules to cross, touch brain tissues, and cause
hypersensitivities, cognitive dysfunction, and other problems (source).
Ammonia can also redistribute cerebral blood flow from cortical to sub-cortical structures
(source).
It could be that ammonium compounds, rather than ammonia per se, are produced by bacteria. For example,
ciguatoxin, which is produced in fish by certain dinoflagellates, is an ammonium compound
(source).
Click here for some general
information about bacterial toxins.
Cytokines produced by the victim's body in response
to bacterial toxins can be a significant component of the Herxheimer reaction.
Some sources recommend cholestyramine to
aid in the binding/elimination of toxins, but other sources oppose it either because they don't
believe cholestyramine works, or because cholestyramine can also bind/eliminate medications and vitamins.
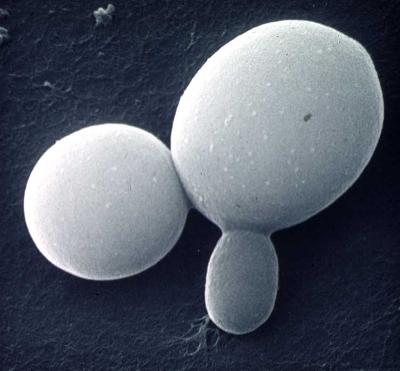
A common side effect of long-term oral antibiotics is proliferation of yeast, mainly Candida albicans,
which is normally a minor fraction of the gut flora but becomes a major part as bacteria - both harmful
and beneficial - are killed. The symptoms of
candidiasis are usually intestinal bloating, cramps, poor digestion, constipation and/or diarrhea.
In advanced cases the normally round yeast can metamorphose into a mycelial form that shoots out filaments
that penetrate into the intestinal walls, thus allowing undigested food, yeast and bacteria that normally
stay in the gut to pass through into the bloodstream (source).
This is called leaky gut syndrome.
There are some dietary modifications that can help keep yeast in check. High-glycemic index foods such as
sugar, white flour and white rice provide easily digestible material for the yeast, resulting in acute
bloating, so these foods should be avoided. You can also take
probiotics to help repopulate
the gut with beneficial bacteria, but these must be of high quality since there is much variation in
cell viability between products. Even with dietary modifications and probiotics, it is still
often necessary to take antifungals such as
fluconazole and
nystatin to reduce the yeast cell count. Even these
aren't always effective, as Candida albicans can form biofilms that make them resistant to
antifungal medications
(source).
Unfortunately, LD can cause the same gastrointestinal disorders listed above
(source),
thus fooling some victims into believing that they have candidiasis when in fact they don't.
There are many substances
that folks who prefer alternative medicine claim will eliminate bacteria or yeast, or boost the immune
system, or help detoxify the body. These claims are hotly debated.
Doubters of alternative supplements cite:
Here are a few examples of alternative supplement health claims:
Some people believe that rife machines
can weaken or kill Bb by exposing them to certain electromagnetic frequencies. Again, it is difficult to tell
whether these claims are true.
In any case,
it is important that sufferers not rely on alternative treatments alone. Bb and Bartonella are elusive,
insidious invaders that need proper medical treatment. Alternative supplements usually do not interfere with
conventional treatment, but if a patient forgoes conventional treatment because he/she believes that
alternative treatment is the answer, that can be dangerous.
Alternative supplements are not as tightly regulated as
pharmaceuticals are. As a result, some do not contain what their labels claim they
contain (source). Additionally, it is known that these products
sometimes contain harmful substances such as heavy metals
(source1
source2).
Some alternative supplements are sold in "homeopathic" concentrations.
Homeopathic preparations are highly diluted substances.
The idea in homeopathy is that just a tiny bit promotes
healing. Less is more, if you will.
This idea seems counterintuitive to many folks, causing it to be another area of debate.
Homeopathic product
labels usually denote potency using either a logarithmic X scale, where the
number in front of the X denotes dilution by a power of 10; or a logarithmic C scale, where the
number in front of the C denotes dilution by a power of 100. For example, 2X is one part in 102,
or a 1% solution. 3X is one part in 103, or a 0.1% solution, and this is actually considered by
many people to be a higher potency than 2X (remember, less is more). This idea is sometimes
taken to such extremes that the dilution makes it improbable that the product contains even a single molecule
of the ingredient. For example, a 60X (30C) product such as
this one would have to be dissolved in
1060 other molecules. That would require a container more than 30 billion times
the size of the Earth. Another example is a supposed flu medication called
Oscillococcinum. It is a 400X (200C)
dilution of duck liver. That's 1 part in 10400. There are only 1080 atoms in the
known universe. Thus, 10320 more universes would be required for there to be the slightest chance
that all the Oscillococcinum on Earth contains even one molecule of duck liver. Homeopaths claim that
molecules of a particular substance leave an "imprint"
in the dilution that causes a healing effect on the body even in the absence of the substance itself,
but available evidence does not support efficacy beyond placebo
(source).
Since the area of alternative medicine is so hotly debated, my (amateur) advice to any vector-borne illness
victim is to take
only those alternative supplements that are prescribed by a VBILMD; don't self-medicate based on the word of
a website or someone working the register at a health food store.
This is not to say that Western medicine is the only treatment for LD, bartonellosis, or any other
disease. While Western medicines might kill pathogens, unconventional substances or treatments can provide
adjunctive support to help the body heal.
Boluoke® contains a fibrin-dissolving
enzyme called lumbrokinase, which is extracted from two species of earthworm
(Lumbricus rubellus and Eisenia fetida). Earthworm has been used in Eastern medicine for many centuries to
treat circulatory problems. Since Bb and Bartonella cause endothelial inflammation that can lead to fibrin
deposits that cause hypoperfusion, lumbrokinase can reverse the process and restore normal nutrient and oxygen
delivery by dissolving those fibrin deposits.
It might also reverse atherosclerosis. Another way in which it can be helpful is in dissolving the
fibrin coating that Bb uses to evade immune recognition. Lumbrokinase
has been thoroughly tested and is deemed safe. The main side effect is that it inhibits
adhesion molecules on platelets, which can cause cuts to bleed more than usual.
Hyperbaric oxygen therapy (HBOT), which
is the medical use of oxygen at greater than normal atmospheric pressure, can be used as a possible way to
help the brain recover. Cerebral hypoperfusion might stun, but not kill, brain cells, and HBOT might stimulate
them back to normal functioning. However, it is not wise to give HBOT to patients before they are bacteria-free
because inflamed tissues can be further damaged by the elevated pressure of HBOT. As for whether HBOT can actually
kill pathogens, this is a matter of debate. The theory is that Bb is a
microaerophile, so it cannot survive HBOT's increased
concentration of oxygen, but the reality is that not all patients subjected to HBOT have improved, and even those
who do improve require several treatments. HBOT is inconvenient, expensive, and often not covered by insurance.
Digesta Guard® is a combination of many strains of Lactobacillus and
Bifidobacterium bacteria. It is supposedly better than store brands at replacing beneficial gut bacteria
that are killed by antibiotics.
Chronic infections can severely limit the body's ability to remove toxic metals such as
lead and mercury (I don't have information on the specific mechanism by which this occurs).
Additionally, antibiotics can inhibit mercury excretion
(source).
Chelation therapy can help
remove toxic metals. There are several chelating agents
such as EDTA,
DMSA and
DMPS. Intravenous
chelation has been proven to reduce blood levels of certain toxic metals, but the effectiveness of oral chelation
is hotly debated. Regardless of effectiveness, chelating agents are apparently safe to use
(source1
source2
source3). However, they can
redistribute rather than eliminate toxic metals
(source), as well as bind and
remove essential minerals such as copper, manganese, molybdenum, iron and zinc. Additionally, EDTA can combine
with iron to have toxic effects (source).
Another possible chelating agent is a type of zeolite called
clinoptilolite. It is sold in both powder and liquid
forms. There is much debate over which form is better, but neither form has been proven effective in clinical
studies.
Vitamin and mineral deficiencies are common in Lyme disease and bartonellosis. These deficiancies may be
indirectly caused. For example, these infections can cause elevated lead levels, and lead impairs calcium
and vitamin D metabolism (source).
A daily multivitamin is
a good idea. Magnesium and vitamins B12 and D are often particularly low, so high doses of
these might be needed. Blood tests to uncover vitamin and mineral deficiencies should be done so that
the patient can take the proper supplements. (If taking calcium, note that most calcium supplements contain
small amounts of lead. Calcium carbonate contains less
lead than dolomite and oyster shell, so read supplements' fine print.)
Anti-oxidants such as N-acetylcysteine,
alpha-lipoic acid,
selenium, etc might provide general health benefits
and therefore help support the Lyme/bartonellosis patient. Vitamins C and E act in synergy with some
anti-oxidants to boost their power.
Omega-3 supplements such as fish oil
and flaxseed oil are beneficial because they help reduce inflammation and they are essential nutrients
that are often lacking in the average diet.
Inflammation can also be reduced by other dietary methods. For example, raw garlic (whose anti-inflammatory
component is allicin) and most teas (which contain
catechins) are two beneficial and readily
available substances (source).
Ornithine might aid the body in eliminating ammonia
(source1
source2), but then again it might not
(source).
GABA supplements might improve
mood and/or sleep for some patients, but this is controversial since GABA does not cross the blood-brain
barrier (source).
Drinking lots of water will help the body flush out toxins.
Sometimes baby aspirin (80 mg) is prescribed as an anticoagulant.
Plenty of rest is necessary when undergoing LD or bartonellosis treatment. These diseases wreak havoc on
the body, and a lot of energy is needed for the body to heal. Tobacco and alcohol are
to be avoided. (source)
Exercise is recommended in order to raise oxygen delivery to hypoperfused tissues. This does not have to
be vigorous exercise. In fact, patients should not push themselves beyond their comfort zone because
inflamed tissues can be further damaged by overwork.
It is imperative that anyone who experiences unexplained muscle/joint aches, fatigue, "fibromyalgia",
"chronic fatigue syndrome", excessive irritability, headaches, abdominal pain, etc
seek help, and to get that help from doctors who are knowledgeable about
vector-borne illnesses. Remember, these symptoms are not necessarily normal effects of aging, and the longer
the bacteria causing them go undetected and untreated, the more damage they will cause and the longer must
be the duration of treatment.
There is a great VBILMD in Rockville Maryland, but for some reason he doesn't
want to be mentioned on this website. One good resource for finding a good VBILMD is
here.
A few Maryland doctors are listed
here.
A Google search will help you find VBILMDs and discussion groups pertaining
to your particular disease(s) where you can ask forum members if they know of a good VBILMD.
Psychiatric help is available for sufferers. Until the pathogens are eliminated and the brain can heal,
patients can be treated for their psychological disorders. However, not just any psychiatrist will
necessarily be able to provide proper treatment, because merely prescribing antidepressants for
pathogenically caused psychological problems can be ineffective or even harmful. Certain psychiatrists
are educated in vector-borne illnesses and can provide appropriate treatment.
Again, a Google search might be of help.
You might have to pay out-of-pocket for good medical help. It is sad but true that insurance companies
are driven by profit, not your health. It is in their interest to ignore or even
deny
the existence of certain diseases. Insurance panels base your health decisions on their profit motive,
not on what will help you get well. Furthermore, the people who make these decisions usually aren't even
doctors. Some patients have had the funding for their antibiotics cut off in the middle of treatment because
their insurance providers deemed the antibiotics to be "unnecessary". Some VBILMDs do not take insurance
because treating an illness that insurers object to can have adverse
consequences. However, there is hope as legislation
is starting to be passed that protects doctors.
The bottom line is that you are ultimately responsible for your own health. If your insurance company
is denying you needed treatment, then either find another insurer or pay for treatment yourself. If your doctor
seems to be ignorant about vector-borne illnesses, then find a better doctor. You owe it to yourself to find
the best treatment possible and not passively accept defeat.
Veterinarians and doctors must work together to combat vector-borne illnesses. Veterinarians have a good amount
of experience in this area since animals tend to remain outdoors longer than humans and hence are more prone to
being infected.
We are lucky to live in this era of information and medicine, when so many previously untreatable ailments
are now treatable. Until recently sufferers of advanced LD and bartonellosis were not so lucky,
but their luck is now turning around.
When to Suspect Lyme
(alternative link
here)
Novel Diagnosis of Lyme Disease: Potential for CAM Intervention
Chronic Lyme Disease and Co-infections: Clinical Overview
Practice Guidelines for the Treatment of Lyme Disease
Healing Lyme Disease: An Integrated Approach to Curing Chronic Infection
Long-Term Inflammation in Lyme Borreliosis
What Every Primary Care Physician Should Know About Lyme Disease
Lyme Toxins the Primary Cause of Your Symptoms
Hemagglutination and Proteoglycan Binding by the Lyme Disease Spirochete, Borrelia burgdorferi
Ticks and Biting Insects Infected with the Etiologic Agent of
Lyme Disease, Borrelia burgdorferi
Advanced Topics in Lyme Disease
The
Psychotropic Management of Late-Stage Lyme and Associated Diseases
Lyme disease statistics by state
An Overview of Bartonella vinsonii subspecies berkhoffii Infection in Dogs
Bartonellosis: Veterinary and Human Implications
Bartonella sp. Bacteremia in Patients with Neurological and Neurocognitive Dysfunction
Ecological fitness and strategies of adaptation of Bartonella
species to their hosts and vectors
Recommendations for Treatment of Human Infections Caused
by Bartonella Species
Entry of Bartonella bacilliformis into Erythrocytes
The World’s Top Stealth Bug Ends Marriages, Friendships and Jobs
Bartonella bacilliformis: Molecular Mechanisms of Invasion
Molecular and Cellular Basis of Bartonella Pathogenesis
Potential for Tick-borne Bartonelloses
Bacteremia in Patients with Neurological and Neurocognitive Dysfunction
Potential Transmission of Bartonella Species by Ticks (212 pages) (Shortened version in Word format)
Bartonella spp. as Emerging Human Pathogens
Natural History of Bartonella Infections
Bartonella: new explanations for old diseases
Bartonellosis: An emerging and potentially hidden epidemic?
Ignore Bartonella and Die - Trivializing Bartonella is Like Ignoring TNT
Bartonella quintana Lipopolysaccharide Is a Natural Antagonist of Toll-Like Receptor 4
An Infection Can Change Your Personality -- There's Plenty of Proof
International Lyme And Associated Diseases Society
NC State University College of Veterinary Medicine
Lyme Disease Research Foundation of Maryland
Lyme and Tick-Borne Diseases Research Center
Fungal Biofilms and Drug Resistance
Neuroprotection by minocycline facilitates significant recovery from spinal
cord injury in mice
Reducing Inflammation With Diet and Supplements:
The Story of Eicosanoid Inhibition
The Impact of 4-Poster Deer Self-Treatment Devices at Three Locations in Maryland
Comments? Suggestions? E-mail lymebartonellosis@yahoo.com
This page had 232,131 hits as of 5/12/2020. The following up-to-date hit counter displays on Internet Explorer and Firefox but not always on Chrome.


Brown dog tick. Left: fully engorged female. Top center: female. Bottom center: larva.
(Source)
Ticks are not the only vectors. Any infected biting creature can transmit a number of diseases.
This includes mosquitoes, fleas, lice, and biting flies
(horse flies and deer flies). (source)
Bites and scratches from infected animals - including pets - can also transmit illnesses.

Flea life cycle. 1: Fed adult. 2: Eggs. 3: Larva. 4: Pupa (covered with dirt).
5: Unfed adult (remains in suspended animation until it detects a host).
(Source)


As mentioned earlier, vectors can transmit several types of parasite. Protozoa of the genus
Babesia
cause babesiosis,
Anaplasma phagocytophilum
causes
human granulocytic anaplasmosis (HGA),
bacteria of the genus
Ehrlichia cause ehrlichiosis,
Rickettsia rickettsii
causes
Rocky Mountain spotted fever,
bacteria of the genus Mycoplasma cause mycoplasmosis,
and Francisella tularensis
causes tularemia.
Thus it is very common for victims to be coinfected.
Polymerase chain reaction
(PCR) tests look for DNA, but this can also
result in false positives or false negatives.
Additionally, if there are children involved, explain to them that their father/mother is ill and that the
harsh treatment they receive from him/her isn't because they've done anything wrong.
For prevention of Lyme disease after a recognized tick bite, routine use of antimicrobial prophlylaxis or serologic testing is not recommended. A single dose of doxycycline (4mg/kgm up to 200 mg) may be offered to adults and to children over 8 yrs of age under the following conditions:
(source)

However, for every claim of a substance's effectiveness, there is a counterclaim. For example:
Nevertheless, many patients insist that alternative supplements have
aided in their recovery. It is often difficult to determine whether improvement in a patient's
condition occurs because of an alternative supplement or it would have happened anyway. Furthermore, it
can also be difficult to determine whether a substance has had any effect other than placebo.
Further reading and resources
As stated previously, the author has no medical training, nor does he purport to offer better medical
information than that offered by medical professionals. The purpose of the information on this
site is to inform, but its accuracy cannot be ascertained.
hits since 9/14/2010